What's actually happening
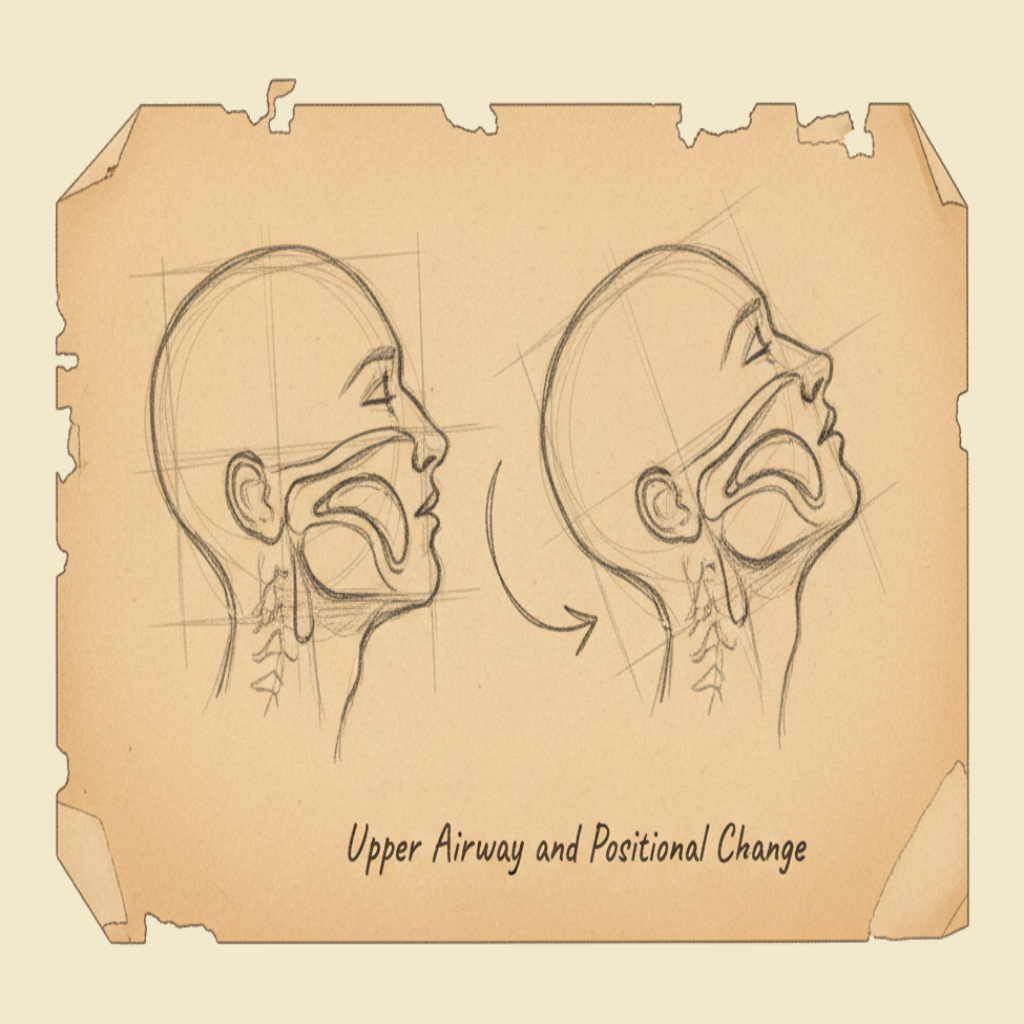
The upper airway is the passage from the mouth and nose down through the throat to the level of the vocal cords — the part of the breathing tract that is open to the outside world. In a conscious, sitting person it stays open by itself: the muscles of the tongue, jaw and pharynx hold their tone, the head sits upright, and air moves freely through it. In an unconscious person on their back, all of this falls apart. The muscle tone is gone, the jaw drops back, the tongue (which is a heavy slab of muscle attached to the lower jaw) slides backwards under gravity, and within seconds the most posterior part of the tongue is sitting against the back of the throat — blocking the airway like a stopper in a bottle. G3 G4
The casualty is now unable to breathe, even though their breathing reflex is still trying to work. From the outside it can look like apnoea, snoring respirations, gasping, or absent breathing. From the inside, the diaphragm is pulling air against a closed obstruction, and the casualty is suffocating in slow motion.
The first aider's intervention for this is so simple it sounds trivial: change the position. Tilt the head back, lift the jaw forward, and the tongue moves with it — opening the airway again. Roll the casualty onto their side and gravity does the same job for the rest of the response. No equipment, no training-intensive technique, no drug. Just position.
§ Instructor's note
The teaching point of this chapter is that positioning is an intervention, not a passive thing the first aider does while waiting for the "real" treatment to begin. A first aider who tilts a head back and gets a casualty breathing again has just done the most important thing of the entire response. Drill the rule: airway first, position is the airway.
The anatomy in two paragraphs
The upper airway runs from two openings — the nose and the mouth — back to a single shared chamber, the pharynx. The pharynx splits at its lower end into two tubes: the oesophagus, which goes down to the stomach behind, and the larynx (the voice box) and trachea, which go down to the lungs in front. Above the larynx sits the epiglottis, a small cartilaginous flap that closes the larynx during swallowing so that food goes the right way. The airway is normally clear, the epiglottis is normally up, and breathing happens without anyone having to think about it.
The tongue is the part that matters most for first aid. It is a single large muscle attached to the floor of the mouth and to the inside of the lower jaw (the mandible). When the casualty is conscious, the tongue's own muscle tone — and the muscle tone of the surrounding pharynx — keeps it forward and out of the airway. When consciousness is lost, the tone is lost, the lower jaw relaxes, and the tongue slides backwards. In a casualty lying face-up on the ground, this is enough to occlude the airway in the great majority of cases. Tilting the head back lifts the lower jaw forward, dragging the tongue with it, and reopens the passage.
The head-tilt / chin-lift manoeuvre
The standard ANZCOR airway opening manoeuvre for a casualty in cardiac arrest is the head-tilt / chin-lift. It is done as follows:
- Place one hand on the casualty's forehead. Apply gentle backward pressure to tilt the head back.
- Place the fingers of the other hand under the bony part of the chin (not the soft tissue under the jaw — pressing there can push the tongue back, the opposite of what you want).
- Lift the chin forward and upward, gently extending the neck.
- Look, listen and feel for breathing — see the recognising unconscious and not breathing chapter.
The manoeuvre takes a couple of seconds and is the entire airway intervention. It does not require equipment, special training beyond this course, or any judgement other than the recognition that the casualty is unresponsive.
If you suspect a spinal injury — a casualty who has fallen from height, been in a vehicle crash, dived into shallow water, or sustained any significant blunt trauma — the recommended manoeuvre changes slightly to jaw thrust, where the lower jaw is pushed forward without tilting the neck. In practice, the ANZCOR position for first aiders is that airway always wins: if you cannot open the airway with jaw thrust alone, you should tilt the head back enough to do so, even with a suspected spinal injury, because a casualty with a clear airway and a possible spinal injury is in a much better position than one with an obstructed airway and a perfect spine. See the head, neck and spinal injuries chapter for the wider context.
The recovery position — gravity as your assistant
For an unresponsive casualty who is breathing normally, the right action is the recovery position. The recovery position is a stable side-lying posture that does three things at once:
- Holds the airway open by letting the tongue fall forward off the back of the throat instead of backwards into it.
- Lets fluids drain out of the mouth — vomit, blood, saliva — instead of pooling in the throat and being inhaled into the lungs.
- Keeps the casualty stable so they don't roll back onto their face or onto their back without you noticing.
The standard ANZCOR recovery-position roll is:
- Kneel beside the casualty on the side you want to roll them toward.
- Place the arm nearest you out at a right angle to their body, palm up.
- Bring the far arm across the chest, with the back of the hand against the casualty's near cheek.
- Bend the far knee up so the foot is flat on the ground.
- Pull on the bent knee to roll the casualty toward you, supporting the head as it comes over.
- Position the head with the cheek resting on the back of the hand and the head slightly tilted to keep the airway open.
- Adjust the bent knee to be at a right angle to the body, propping the casualty in a stable side position.
- Re-check breathing every couple of minutes while you wait for the ambulance.
There are slight variations — some traditions cross the arms, some position the legs differently — and they all work. The point is that the casualty ends up on their side, stable, with their head slightly tilted and their face slightly downwards, so the airway stays open and any vomit can drain out instead of in.
Children, infants and the airway position
The airway anatomy of a child is similar to an adult; an infant (under one year old) is meaningfully different. Infants have proportionally larger heads, shorter necks, larger tongues relative to the mouth, more pliable cartilage in the larynx, and a higher larynx that sits closer to the base of the tongue. The practical consequences for the first aider:
- For an infant, a neutral or only slightly extended head position is correct — over-extending the neck can actually obstruct the infant's softer airway, the opposite of the adult situation. Imagine you are sniffing — that's about the right position for an infant.
- For a child of about one year and older, the adult head-tilt / chin-lift works as for an adult, with proportionally less force.
- The recovery position works for children and infants with the same logic as for adults — side-lying, head tilted slightly, body supported.
These differences are covered in more detail in the CPR anatomy for adults, children and infants chapter.
What positional change actually achieves
If you take one thing away from this chapter, take the following: changing the position of an unresponsive casualty is the difference between an open airway and an obstructed one. Almost every other intervention in CPR — compressions, breaths, AED — depends on the airway being open in the first place. Position is not a preliminary; it is the foundation.
Concrete cases where position is everything:
- An unconscious-but-breathing casualty face-up — at risk of airway obstruction by the tongue, and at risk of aspiration if they vomit. The recovery position fixes both.
- A drowned casualty pulled from the water — their stomach is full of water, they are likely to vomit, and the recovery position protects the airway. See the drowning chapter.
- A post-ictal casualty after a seizure — they are in a deep sleep-like state, the tongue has lost tone, the airway is at risk. Recovery position. See the seizures chapter.
- An intoxicated casualty asleep on their back — same problem, same solution. The recovery position has saved more lives in pubs and dorm rooms than any other first-aid intervention.
- A diabetic casualty in a hypo who has lost consciousness — recovery position, then call for help.
- A casualty in cardiac arrest — head-tilt / chin-lift to open the airway, then begin CPR. See below.
In every one of these, the casualty's outcome is largely determined by whether the airway is open in the first few minutes — and the airway being open depends, almost entirely, on the position.
Position and the cardiac arrest casualty
A casualty in cardiac arrest is in a special category: they need CPR first, not the recovery position. CPR is performed with the casualty face-up on a firm surface, with the airway opened by head-tilt / chin-lift, and with chest compressions as the central intervention. The recovery position is for casualties who are unconscious but breathing normally; the cardiac arrest casualty is, by definition, not breathing normally and needs the active intervention.
The decision flow is:
- Check responsiveness — shout, shake, no response.
- Open the airway — head-tilt / chin-lift.
- Check breathing — look, listen, feel for up to 10 seconds.
- If breathing normally — recovery position, monitor, call for help.
- If not breathing normally — call for help, start CPR with the casualty face-up.
The choice between "recovery position" and "CPR" is made on this single observation: is the casualty breathing normally or not? Both pathways start with opening the airway by changing the position; only the next step differs.
In the first minute or two of cardiac arrest, many casualties have agonal breaths — slow, irregular, gasping, snoring, or sighing breaths that can fool a bystander into thinking the casualty is "breathing okay". They are not. Agonal breaths are a brainstem death rattle and are a sign of cardiac arrest, not a sign of life. If a casualty is unresponsive and the breathing is anything other than normal, regular breathing, treat them as not breathing and start CPR. See the recognising unconscious and not breathing chapter.
When position alone isn't enough
The head-tilt / chin-lift and the recovery position handle the vast majority of upper-airway problems a first aider will encounter. They do not handle:
- Foreign body airway obstruction (choking) — the airway is blocked by an object, not by the tongue. The intervention is back blows and chest thrusts. See the choking chapter.
- Severe anaphylaxis with airway swelling — the soft tissues of the throat and tongue are swelling from the allergic reaction. The intervention is adrenaline. See the anaphylaxis chapter.
- Severe burns to the face and airway — the tissues are oedematous from heat injury. Position helps a little; the casualty needs paramedic-level airway management urgently.
- Trauma with massive bleeding into the airway — blood is filling the airway from above. Recovery position helps drainage; the casualty needs urgent paramedic intervention.
In all of these, position remains a useful adjunct — recovery position to drain fluids, head-tilt to maximise the patent airway you have — but it isn't the primary fix, and the call to 000 is urgent.
Listen to a casualty's breathing while you have your face close to theirs. Snoring sounds in an unconscious casualty almost always mean the tongue is partly obstructing the airway — open the airway with head-tilt / chin-lift and the snoring should stop. Gurgling sounds usually mean fluid in the airway — turn them onto their side and let it drain. Stridor — a high-pitched harsh sound on inspiration — means partial obstruction at or near the larynx and is a severe finding that needs urgent medical care. Each sound tells you something useful about what the airway is doing.
The airway should be opened by tilting the head back and lifting the chin forward (head-tilt / chin-lift). For unresponsive casualties who are breathing normally, the casualty should be placed in a stable side-lying position (the recovery position) to maintain a clear airway and reduce the risk of aspiration. For infants under one year, the head should be kept in a neutral position. Where spinal injury is suspected, jaw thrust may be used as an alternative manoeuvre, but maintaining a clear airway always takes precedence over concerns about spinal movement.
What not to do
- Do not leave an unresponsive but breathing casualty face-up. Recovery position, every time.
- Do not put a pillow under the head of an unconscious casualty — it flexes the neck and tends to obstruct the airway.
- Do not press on the soft tissue under the jaw when doing chin-lift; lift the bony chin only.
- Do not over-extend the neck of an infant — neutral or slight extension is correct.
- Do not delay CPR because of concern about spinal injury — airway and breathing always take precedence.
- Do not ignore snoring or gurgling sounds in an unconscious casualty — they are telling you the airway is partly obstructed.
You will rehearse the head-tilt / chin-lift on a manikin and the recovery-position roll on a partner, until both are smooth, automatic, and quick. The roll is one of the most useful single skills in this course — it works on a drunk friend at a party, an unconscious colleague at work, an injured stranger by the side of the road. By the end of the day it should feel like something your hands know how to do without your brain having to coach them.
The cheapest, fastest, most reliable airway intervention in first aid is to change the position of the casualty's body. Tilt the head, lift the chin, roll them onto their side — three movements that handle the great majority of upper-airway problems with no equipment and no training beyond this chapter. Position is the airway.
— ANZCOR Guideline 4 (Airway)